Tennis elbow, technically known as lateral epicondylitis, is experienced as pain over the lateral (outside) part of the elbow. It affects about 1-3% of the general population, and usually occurs in people between 35-45 years old. It is experienced when there is degeneration, tendonosis, and periostitis at the common extensor tendon and lateral epicondyle of the humerus.
Causes And Pathology
The lateral epicondyle serves as a bony anchor to which the wrist extensors are attached. The main muscle involved is the extensor carpi radialis brevis (ECRB), but there may also be involvement of other muscles including the extensor carpi radialis longus (ECRL), extensor digitorum, and supinator.
Although it is called “tennis” elbow, it is not necessarily caused by playing tennis or any other sport. Instead, it is usually caused by overuse of the wrist extensor muscles. These are the muscles on the dorsal (back side) of the forearm, and they can be overused in many repetitive tasks, especially typing and using a mouse.
Tendinopathy is defined as pain and dysfunction in the tendon, caused by a failed healing response of the tendon. Tendons are what connect muscles to bone, and overuse of the muscle can cause injury to the tendon. The body attempts to heal this injury through an inflammatory response, which in the short run is known as tendonitis. If it doesn’t succeed in healing, longer term changes can result which include disruption of collagen fibers, collagen disorganization, and neurovascular ingrowth.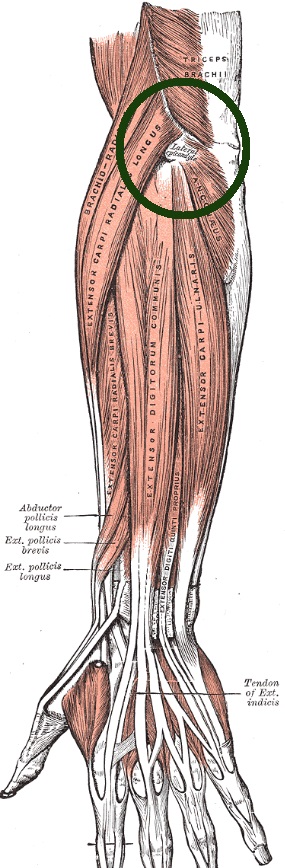
Signs and Symptoms
Tennis elbow usually presents with a gradual onset of intermittent pain in the elbow. It may also present with pain and weakness with grasping and twisting motions, such as turning a door handle. Sometimes it is severe enough to wake the patient at night.
Diagnosis
Physical examination will reveal tenderness to palpation at the lateral epicondyle and tendon origin, but not usually swelling. The patient will experience pain at the lateral epicondyle with resisted middle finger extension or resisted wrist extension (Cozen’s test). Some other conditions which may present similar symptoms include radial tunnel syndrome, posterior interosseus nerve syndrome, elbow osteoarthritis, and cervical radiculopathy. Imaging is not usually done at first, but long standing cases may be investigated further with ultrasound, x-ray, or EMG to rule out nerve compression.
Conventional Treatment
Conservative treatment may involve the use of NSAIDS for relieving pain and inflammation in the short term. Ice is has also been found to be useful. A counterforce brace may be applied around the forearm to reduce tension on the wrist extensors. Corticosteroid injections may also be given, as well as physical therapy stretching and exercises.
Acupuncture Treatment
We treat many patients with lateral epicondylitis. Our treatment always begins with examining the motion of the elbow, as well as the wrist, shoulder and neck. The goal is to first improve motion in the joints, then reduce pain in the affected areas. The treatment involves using acupuncture to first reduce tension in the muscles attached to the elbow, and secondly to relieve pain and inflammation at the elbow itself. We combine it with soft tissue techniques (gua sha and tui na), and taping.
The muscles involved in lateral epicondylitis are mainly wrist extensors. These include the extensor carpi radialis brevis, extensor carpi radialis longus, extensor digitorum communis. Additionally, other trigger points relevant to the area may be found in the anconeus, triceps, and brachioradialis. Also, we may uncover imbalances further up the myofascial chain, including in the shoulder and cervical area.
Each treatment takes 30-40 minutes, and is repeated once or twice per week depending on severity and chronicity. Recovery depends on how severe the pain is and how heavily the arm is used, but 4-8 treatments should produce relief. If no relief is obtained, we refer to an orthopedic physician for further evaluation.
Sources
Vizniak, Nikita. Conditions Manual. Professional Health Systems, Inc., 2010
Hertlin, Darlene, and Kessler, Randolph. Management of Common Musculoskeletal Disorders, Physical Therapy Principles and Methods 3rd Edition, Philadelphia, Lippincott, 1996
Reaves, Whitfield with Bong, Chad. The Acupuncture Handbook of Sports Injuries and Pain, A Four Step Approach to Treatment, Boulder, CO, Hidden Needle Press 2009
Callison, Matt. Sports Medicine Acupuncture: An Integrated Approach Combining Sports Medicine And Traditional Chinese Medicine, San Diego, AcuSport Education 2019
This information is for educational purposes only and is not intended to replace the advice of your doctor. Naperville Acupuncture Center disclaims any liability for the decisions you make based on this information. The information contained on this website does not establish, nor does it imply, doctor-patient relationship. Naperville Acupuncture Center does not offer this information for diagnostic purposes. A diagnosis must be provided by a licensed physician and is not assumed based on the information provided.