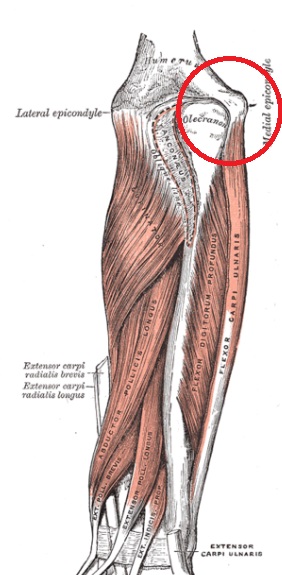
Medial epicondylitis, or ‘golfer’s elbow,’ is experienced as pain at the medial (or inside) of the elbow. This is in opposition to lateral epicondylitis, or “tennis elbow,” which is on the lateral, or outside of the elbow. It occurs at the origin of the common flexor tendon, and especially involves the pronator teres. Sometimes there is also pain on the ulnar(little finger) side of the forearm, the wrist, and occasionally in the fingers.
Causes and Pathology
It is mostly due to tendinous overload, which leads to tendinopathy. Degeneration of the flexor/pronator tendon happens with repetitive forced wrist extension and forearm supination. These motions are involved with overhand throwing, serving a tennis ball, swinging a golf club and using a hammer.
Despite the suffix “-itis,”, this is not technically an inflammatory problem. Instead, it is a cellular problem. In tendinopathy, Wear and tear mechanically breaks down the tendon. The body attempts to heal but cannot keep up with the continuous usage. This usually results in an abnormal arrangement of collagen fibers. There can also be an increased vascularization (blood vessel formation), and necrosis or calcification.
What this basically means is that the tissue has healed improperly and as a result loses its strength. It becomes fragile and easily injured. With each successive injury, the collagen breaks down, and the body responds by forming scar tissue in the tendon. Eventually, the tendon becomes thickened from extra scar tissue (tendinosis). The appearance and quality of the tendon actually changes from a white, glistening and firm to dull, brownish and soft.
Diagnosis
The diagnosis of medial epicondylopathy is based on local pain at the elbow, tenderness and pain with palpation distal and anterior of the medial epicondyle. An increase in pain at the medial epicondyle with resisted isometric flexion, repetitive flexion and pronation of the wrist can be found in examination.
Conventional Treatment
Conservative treatment (non-surgical) usually involves rest, ice, compression, NSAIDS or steroid injection, followed by physical therapy including stretching and exercise. More serious cases may require surgical treatment, such as a mini-open muscle resection procedure or a fascial elevation and tendon origin resection.
Acupuncture Treatment
The acupuncture treatment begins with an assessment not only of the elbow but also the neck and shoulder. Muscle length, strength, and joint motion are assessed. Motor points from muscles including the pronator teres, flexor carpi ulnaris, and palmaris longus are stimulated to improve their function and reduce tension on the elbow. Additional points in the shoulder girdle and neck may be selected to improve overall motion and circulation in the arm. Electrical stimulation may be done to the bony part of the elbow to reduce pain. Tui Na (Traditional Chinese Medicine massage) techniques may also be included, as well as sports taping. Finally, dietary and exercise suggestions may be offered.
For most cases, acupuncture treatments are effective at reducing pain and increasing function. Depending on how severe and chronic the case is, it may reach maximum improvement in anywhere from 4-10 visits. If there is no improvement, imaging should be done to rule out osseous changes or angiofibroblastic degeneration.